

.png)


If you have COPD, then you've probably realized that treating the disease is not a simple process. In order to get it right, your doctor needs to have a very thorough understanding of your physical condition and the nature of your disease.
Because of this, people with COPD have to undergo a large number of medical tests and screenings over the course of COPD treatment. These tests, which include blood screenings, x-rays, spirometry measurements, and more, allow your doctor to tailor your treatment plan specifically to your needs.
Unfortunately, while these tests reveal valuable information about your health and your disease, many patients don't fully understand what their results mean. Even if you have a general idea of what the tests are for, chances are you still wouldn't know how to read and understand the results.
Fortunately, you don't have to be a doctor or a nurse to make some sense out of your medical test results. With a little practice and help, just about everyone is capable of grasping the important aspects of the different tests used to diagnose and monitor COPD.
In this post, we're going to teach you all about these tests—lung function tests, blood tests, chest scans, and more—and show you how to interpret the data in the results. We'll explain what each test is, how it works, and how to figure out what your results actually mean for you and your health.
This is a useful skill that can help you better understand what's going on when you visit your doctor and work with other members of your COPD treatment team. It can also give you the confidence to ask more questions and understand the nuances of treating and monitoring your disease.
Even though the medical jargon can seem complicated at first, it won't seem nearly as intimidating once it's broken down into layman's terms. Once you learn the basics, you'll find it much easier to navigate the medical vocabulary surrounding your disease and treatments.
In the following sections, we'll give you the information you need to start understanding your COPD test results on a deeper level than before. That way, you can take a more active role in your health and treating your COPD.
Getting Your Hands on Your COPD Test Results

Image from Weiss & Paarz www.weisspaarz.com
If you want the opportunity to understand what your COPD tests mean, you need to make sure you have ready access to your results. In some cases, this is as simple as asking your doctor to give you a copy of all your records and reports.
Some healthcare providers, on the other hand, may require you to follow a specific request process in order to get your records. You may need to write a letter, fill out a form, or pay a small fee to cover the cost of making copies and mailing.
Whenever you take a new spirometry test or another type of health screening, make sure to let your doctor know that you'd like to look at the results yourself. Some test results take days or weeks to come
back, but if your doctor knows you're waiting to see them, he can make sure you get access to the records as soon as they're available.
Also keep in mind, that, if you live in the US, you are always entitled to see and review your medical records by law, except in a few rare cases (usually related to mental health records). It is a right under the US Health Insurance Portability Accountability Act (HIPAA), and it states that you must be able to access existing records within 60 days of requesting them.
If you cannot access your medical records or feel that your rights to review your records have been violated, you can file a complaint with the US Department of Health and Human Services. Just make sure you file your complaint with 180 days of your denied request.

Leverage Your Doctor's Experience: Always Listen to the Expert

Whenever possible, you should ask your doctor to go over your COPD test results with you personally, especially if you are unfamiliar with the test or how the data is organized. Even if you know the basics of what you're looking at, your doctor can help you understand the report much better than you could on your own.
You might ask your doctor to go through the report with you line-by-line to help guide you through the information. This gives him the chance to explain important concepts and details that can help you better interpret the results.
This also gives you an opportunity to ask questions and express any concerns you have about the results of your test. If there's anything you are unsure of, don't be afraid to ask your doctor to explain it more clearly.
Understanding Your Lung Function Test Results
There are several different types of lung function tests (also known as pulmonary function tests), and their purpose is to measure how well your lungs are working. They are quick, reliable, and simple to do, which is why they are widely used both to diagnose COPD and to monitor the disease long term.
Lung function tests can tell you whether or not your lungs are damaged and, if they are, give you a better idea of how much damage they have sustained. Doctors use the results to both diagnose COPD and to gauge the severity of the disease.
If you have COPD, then it's important to familiarize yourself with lung function tests—especially spirometry—and how they work. You will take them fairly often over the course of your treatment, likely as part of your regular COPD check-ups.
Taking these tests periodically allows your doctor to track any changes that happen in your lung function over time. This is important, because it allows your doctor to catch and treat problems, like infections, exacerbations, and lung function decline quickly when they occur.
The results of your lung function tests also help your doctor decide what kinds of medications and treatments you need. They also help your doctor determine how well your current treatments are working and evaluate the effectiveness of newly-prescribed medications.
Spirometry
Spirometry is the primary method doctors use to measure lung function and evaluate COPD. It's a relatively simple test that measures changes in your lung volume as you breathe.
By measuring these changes, spirometry can evaluate whether or not your airways are obstructed, and if they are, to what degree. Because of this, spirometry measurements are a reliable way to diagnose COPD and determine how severe the disease is.
Spirometry tests are simple, painless, and relatively quick to complete. If you have COPD, your doctor will probably ask you take a spirometry test at every appointment so that he can look for any changes in your results.
Taking a Spirometry Test

In order to take a spirometry test, you have to breathe out through a mouthpiece attached to a small machine called a spirometer. Your doctor will also put a clip on your nose to pinch your nostrils shut; this is simply to make sure that you only breathe through the mouthpiece during the test.
Then, your doctor will instruct you to take in a deep breath of air (not through the mouthpiece) before exhaling as forcefully and completely as you can into the spirometer's mouthpiece. You will need to do this at least a few times or until your doctor gets a good set of clean results.
The entire process should take less than fifteen minutes to complete. However, you may need to take the test two separate times: once without taking any medication, and once after you've used a bronchodilator inhaler, with a short pause in-between.
This is known as a bronchodilator reversibility test because it tells you how much the bronchodilator medication is able to improve your airway obstruction. This tells your doctor how well you respond to the medication and helps him determine the best course of treatment.
Spirometry Test Measurements
There are three main measurements that your doctor will measure in a typical spirometry test:
- FVC: Forced Vital Capacity
- FEV1: Forced Expiratory Volume (in one second)
- FEV1/FVC: this is a ratio comparing your forced expiratory volume (FEV) to your forced vital capacity (FVC)
Spirometry tests take other measurements as well, including forced expiratory flow (FEF), peak expiratory flow rate (PEFR), and maximal voluntary ventilation (MVV). However, we're not going to discuss these in any detail here because FVC, FEV1, and FEV1/FVC are usually the most important spirometry results to look at when it comes to diagnosing and monitoring COPD.
FVC: Your forced vital capacity (FVC) essentially tells you how much air you can push out of your lungs in one breath. More specifically, it is a measure of how much air (in volume) that you can exhale forcefully and quickly from your lungs after taking in as deep a breath as you can.
FEV1: Your FEV1 tells you how much air you can exhale from your lungs in exactly one second after taking a deep breath. Basically, FVC tells you the volume of air you push out during one full exhale, while FEV1 tells you the volume of air you can push out during the first second of that full exhale.
FEV1/FVC: When you divide your FEV1 by your FVC, you get another important number, which is simply referred to as your FEV1/FVC. This tells you what percentage of the air you exhaled from your lungs was pushed out during the first second of your exhale.
For example, an FEV1/FVC of 90% means that you pushed out 90% of the air during the first second of your exhale, and the remaining 10% of the air after that first second. If your FEV1/FVC percentage is too low, it is a sign that something is preventing you from pushing the air out of your lungs as quickly as you should.
If your FEV1 or FVC results are abnormal, this FEV1/FVC ratio helps your doctor determine whether or not the abnormality is caused by an obstruction (e.g. COPD) or a restrictive lung disease (in which FEV1 and FVC should change at a similar rate). If you have an FEV1/FVC of 80% or less, it is a strong sign that you have an obstructive lung disease.
Interpreting Spirometry Results
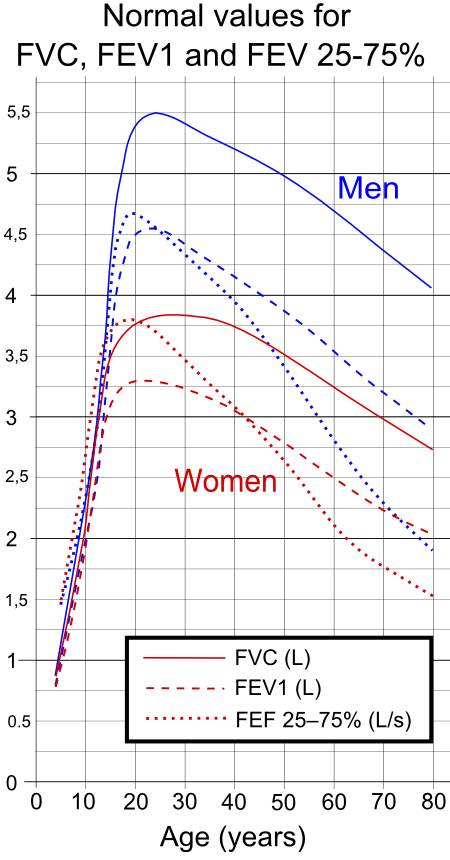
In order to make sense of your spirometry test results, you need to compare them against a standard table of healthy FEV1 and FEV1/FVC values. This will tell you how much your numbers differ from numbers collected from healthy adults of your age, weight, and height.
Then, in order to truly understand what these numbers mean, you will need to refer to another table, known as the GOLD spirometric criteria for COPD severity. This table presents four different ranges of FEV1 and FEV1/FEC results and tells you what it means if your numbers fall within that range.
The GOLD guidelines are the most commonly used and widely accepted criteria for diagnosing COPD. Finding out where your results fall within these four GOLD categories will tell you what stage of the disease you have and give you a better idea of how severe your COPD is.
Here's a quick look at the GOLD guidelines and what they can tell you about your health.
GOLD Spirometric Criteria for COPD Severity
- Stage I: Mild COPD
- FEV1/FEC less than 0.7
- FEV1 greater than or equal to 80%
- Stage II: Moderate COPD
- FEV1/FEC less than 0.7
- FEV1 between 50% and 80%
- Stage III: Severe COPD
- FEC1/FEC less than 0.7
- FEV1 between 30% and 50%
- Stage IV: Very Severe COPD
- FEV1/FEC less than 0.7
- FEV1 less than 30% or less than 50% plus chronic respiratory failure
While it's important to read and understand your spirometry test results yourself, remember that only your doctor has the training and expertise to accurately interpret the results. A licensed doctor is the only one qualified to diagnose COPD or make the call on what stage of the disease you have.
Lung Plethysmography

Lung plethysmography (pronounced ple-thiz-mah-graf-ey) is a test that measures your lung capacity, or how much air your lungs can hold at one time. It can also tell you how much air is left in your lungs after you exhale.
Your lung capacity is closely related to your general lung function, which is why plethysmography is often used to evaluate and monitor COPD. In particular, plethysmography helps your doctor determine whether or not your airways are obstructed, and how much they are obstructed, by measuring how you breathe.
This is especially useful for diagnosing unknown breathing problems, because it can confirm or rule out airway obstruction as a cause. This helps doctors determine whether someone has COPD or different type of breathing disorder.
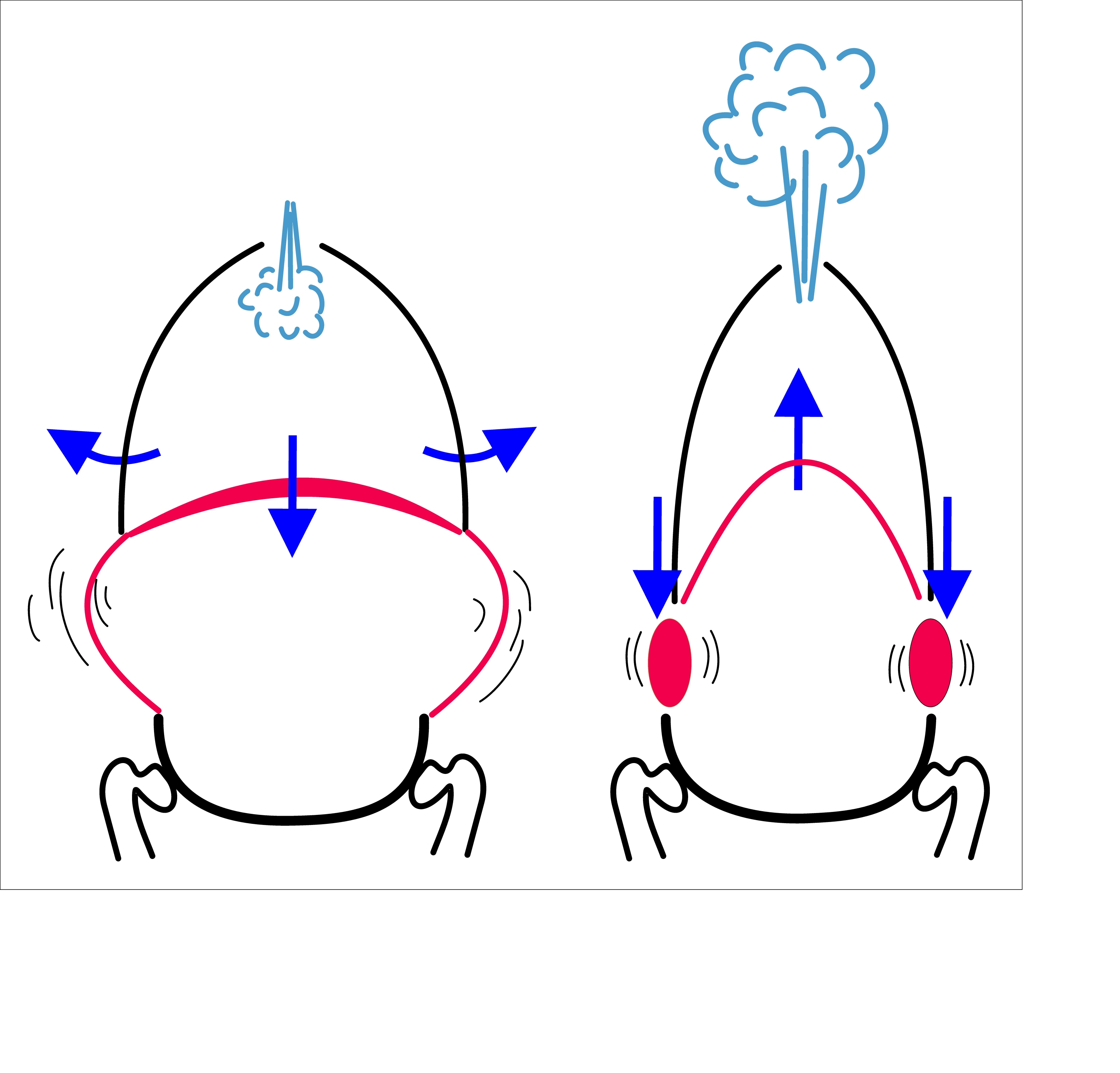
Lung plethysmography also allows your doctor determine whether or not your lungs trap air and how severe the problem is. It does this by measuring exactly how much air is left in your lungs after you exhale.
This is important, because trapped air is a very common problem for people with COPD, and it can significantly worsen respiratory symptoms. Trapped air makes it difficult to breathe, worsens shortness of breath, and can actually stretch out your lung tissue (causing hyperinflation) over time.
Taking a Lung Plethysmography Test
 |
| Photo by Airman 1st Class Teresa Cleveland |
Taking a lung plethysmography test is simple and usually only takes about fifteen minutes to complete. All you have to do is sit in an enclosed, transparent chamber (about the size of a phone booth) and breathe in and out through a special mouthpiece attached to a spirometer machine.
During the test, your doctor will instruct you to breathe in specific ways so that the machine can measure a wide range of breathing patterns. You will alternate between normal breathing, fast breathing, shallow breathing, deep breathing, and any other breathing patterns your doctor wants to test.
If you normally use oxygen, you will most likely be instructed not to use it during the test. You may also stop the test and leave the chamber at any time if you feel too uncomfortable or claustrophobic, though this may require you start the test again from the beginning.
Interpreting Your Lung Plethysmography Results

Throughout the test, the machine attached to your mouthpiece carefully measures the airflow in and out of your lungs. The results provide your doctor with a few very important pieces of information about your lungs and how you breathe.
Specifically, there are three main things the test can tell you about your lungs:
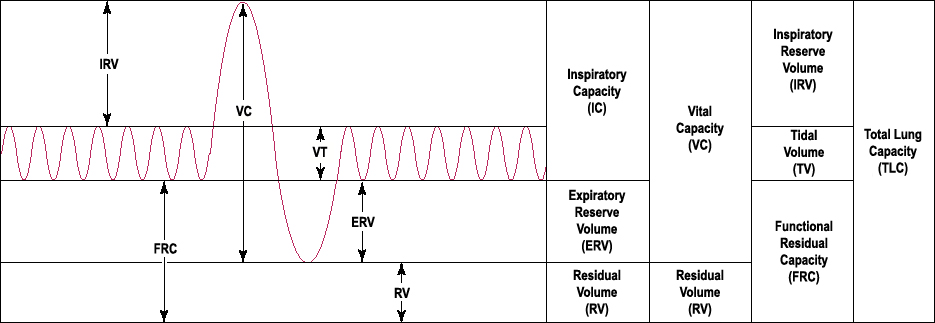
- Total Lung Capacity (TLC): the amount of air in your lungs after you breathe in as deeply and fully as you can
- Functional Residual Volume (FRV): the amount of air that is left in your lungs after exhaling as fully and completely as you can
- Functional Residual Capacity (FRC): this is a measure that compares the amount of air left in your lungs after a normal exhale to the amount of air left in your lungs after you exhale as fully and completely as you can
To understand what these results mean, you will have to compare the numbers from your results to the numbers that are considered healthy for your age, sex, height, and weight. If your results are equal to the healthy standard, then that indicates that your results are normal. If your numbers are significantly higher or lower, however, that indicates abnormal lung function.
You can use the information in the following sections as a basic guide to help you understand how to interpret your plethysmography results when comparing them to the healthy standard:
Total Lung Capacity (TLC)
Increased TLC: If your total lung capacity is higher than normal, this can be a sign of a lung disease like emphysema. It means that your lungs can hold more air than the average person, which is often caused by obstructive lung diseases and especially lung hyperinflation.
Decreased TLC: It is a bad sign if your total lung capacity is lower than normal because it indicates that your lungs are not able to expand or fill up as much as they should. This is often caused by restrictive lung diseases like pulmonary fibrosis, which are different from obstructive lung diseases like COPD.
Functional Residual Volume (FRV)
Increased FRV: If your functional residual volume is higher than the healthy standard, it is a bad sign because it means that there is too much air left in your lungs even after you exhale completely. This is a sign that your lungs have lost elasticity and/or are hyper-inflated, which is common in people with COPD and especially emphysema.
Functional Residual Capacity (FRC)
Increased FRC: It is a bad sign if your FRC numbers are higher than the healthy standard because it indicates that air stays trapped in your lungs after you exhale. The higher the number, the more severe the problem is.
This indicates that you suffer from an obstructive lung condition, and is very common in people with COPD.
Decreased FRC: It is also a bad sign if your FRC numbers are lower than the healthy standard, because it means that your lungs are not filling up as much as they should. This indicates that the amount of available airspace in your lungs is reduced, which is often caused by narrowed airways and/or loss of elasticity in the lungs.
Decreased FRC is common in people with pulmonary fibrosis, sarcoidosis, obesity, and in people who have had lung reduction surgeries or strokes.
Lung Diffusion Tests
 |
| Image from Medical Graphics |
Whereas spirometry tests measure your lungs' overall strength, lung diffusion tests (also known as gas diffusion studies) specifically measure gas exchange, or how well your lungs can transfer gasses to and from your bloodstream. That is the lungs' primary purpose, after all: to absorb oxygen into your blood and remove carbon dioxide from it.
Your lungs do this via millions of tiny air sacs, called alveoli, which fill up with air when you breathe in. These alveoli are covered in tiny blood vessels with walls thin enough that gasses (oxygen and carbon dioxide) can passively move, or diffuse, in and out of the blood.

However, if these air sacs become damaged, then gasses cannot diffuse through them as easily, if at all. This type of lung damage is permanent and it is one of the defining characteristics of emphysema, one of the two main types of COPD.
In people with COPD, this lung damage continues to get worse and spread as the disease progresses. As more and more alveoli become damaged, less oxygen can diffuse into your bloodstream and less carbon dioxide can diffuse out.
That's why doctors perform diffusion tests on people with COPD and other lung disorders. By measuring how well gasses can diffuse through the alveoli in your lungs, diffusion tests help your doctor determine the nature and extent of any lung damage you have.
Taking a Lung Diffusion Test

Diffusion tests work like this: first, you breathe in a specially-formulated gas mixture through a mouthpiece and tube attached to a spirometer machine. This gas mixture is harmless and contains a specific amount of a “tracer gas,” usually carbon monoxide, which your lungs will process after you breathe it in.
Next, you hold your breath for about ten seconds in order to give the gas time to diffuse through your alveoli and get absorbed into your bloodstream. Then, you breathe out through the mouthpiece, which will deliver the exhaled air to the spirometer machine for analysis.
The machine then measures precisely how much carbon monoxide is in the air you exhaled. The more carbon monoxide left in the air, the less your lungs were able to absorb.
Essentially, healthier lungs will exhale less carbon monoxide, while damaged lungs will exhale more. The results of the test represent your lungs' diffusing capacity, often abbreviated with the acronym DLCO.
Your DLCO gives you a more precise ideas of how well oxygen and carbon dioxide can diffuse through your alveoli when you breathe. For example, if your lungs can't process the carbon monoxide very well, that means they cannot process oxygen or carbon dioxide well either.
Interpreting Your Lung Diffusion Test Results
To interpret your individual results, your doctor will compare your DLCO with the healthy standard for someone of your age, sex, and height. A DLCO that is 60 to 80 percent of what is expected from healthy lungs indicates reduced lung function. A DLCO less than 40 percent of what is expected indicates severe lung function impairment.
Diffusion tests are particularly useful for measuring the extent of lung function decline because they measure the lungs' ability to do their job in such a direct way. Because of this, doctors perform diffusion tests often both to diagnose lung diseases and to monitor existing health conditions like heart disease and COPD.
Pulse Oximetry Tests

Pulse oximetry is a simple test that measures the levels of oxygen in your blood. This serves as an indirect measure of lung function as well, since the amount of oxygen in your bloodstream is directly affected by how much oxygen your lungs absorb.
More precisely, a pulse oximetry test tells you your blood oxygen saturation. This number tells you what percentage of red blood cells in your arteries (the blood vessels which carry oxygen-rich blood from the lungs) are carrying oxygen.
This gives you an idea of how well your lungs are able to keep up with your oxygen needs. High saturation is a sign of good lung function, while low saturation indicates poor lung function in people with COPD.
This helps your doctor track the severity of your disease and how well your treatments are working to manage your COPD. It also allows your doctor to watch for chronic hypoxemia and determine how to treat it when it occurs.
Because pulse oximetry tests are so easy to do, your doctor will likely measure your blood oxygen saturation at every check-up and visit. If you use oxygen or suffer from very severe COPD, you may even benefit from getting a personal pulse oximeter to use at home.
Home pulse oximeters help some patients learn how to use their supplemental oxygen better by allowing them to tell when their blood oxygen levels drop throughout the day. They can also warn you if your blood oxygen saturation levels fall low enough to cause hypoxia, a dangerous and life-threatening condition that requires immediate medical attention.
Taking a Pulse Oximetry Test

When you take a pulse oximetry test, you will probably use a tool called a finger pulse oximeter. This is a tiny, clamp-like device, about a few inches long, that is designed to clip directly on to the tip of your finger.
The top part of the clamp has a small infrared laser and often a digital screen to display the test results (some are attached via cable to a separate read-out screen). The pulse oximeter reads your blood oxygen saturation by shining the infrared light through the top of your finger and through the arteries carrying blood underneath.
Then, the pulse oximeter measures the amount of light that comes through the bottom side of your finger, which allows it to calculate the amount of oxygen in the arteries the light passed through. This works because red blood cells carrying oxygen absorb more infrared light than empty, oxygen-less red blood cells.
All of this is completely painless and usually takes only seconds to complete. You simply clamp the device to the end of your finger and wait several seconds until the results appear on the display screen.
In some cases, you will need to leave the pulse oximeter on your finger in order to measure your blood oxygen saturation over a longer period of time. This is useful for a variety of things, including monitoring critically ill and hospitalized patients and measuring changes in oxygen levels during physical exercise tests.
Interpreting Your Pulse Oximetry Test Results
When you read your pulse oximetry results, look for the number representing your SpO2, which is your blood oxygen saturation. It is usually written as a percentage or a decimal which you can convert into a percent.
For example, let's say you got a pulse oximetry reading of 94%. That means that 94% of the red blood cells in arteries are oxygenated, while 6% are not.
A high blood oxygen saturation level indicates your lungs are doing a good job of absorbing enough oxygen into your bloodstream. On the other hand, a low blood oxygen saturation level means your lungs aren't able to absorb oxygen fast enough to keep up with your body's oxygen needs.
Here's a quick guide to understanding your blood oxygen saturation readings:
- SpO2 greater than 94%: generally considered healthy
- SpO2 less than 94%: generally considered abnormal; indicates mild hypoxemia
- SpO2 less than 90%: abnormal, unhealthy, and might mean that you have chronic hypoxemia; often requires supplemental oxygen therapy to correct
Some pulse oximeters also measure your heart rate which, in some cases, can give you a bit more information about your lung function than your SpO2 alone. In general, a healthy heart rate should be between 60 and 100 beats per minute at rest, but it's better to have a resting heart rate in lower end of that range.
If your resting heart rate is too high, it might be a sign that your heart is pumping harder in order to compensate for poorly-functioning lungs. This is especially likely for people with COPD who have a high heart rate paired with normal blood oxygen saturation.
If your heart rate is high and your blood oxygen saturation is low, then this could indicate the same problem, except that your heart's extra work isn't enough to compensate for your lungs' limitations. However, it's important to note that one pulse oximetry reading is not enough on its own to know this for sure.
In order to accurately interpret your results, your doctor will need to consider the results of multiple pulse oximetry tests taken at different times. Then, he will need to compare these to other lung function measurements in order to get a fuller picture of what they mean.
If you have COPD and your blood oxygen saturation is below 90%, then you may need to begin supplemental oxygen therapy. Even if your oxygen levels don't stay that low all the time, you might need to use supplemental oxygen when you sleep, exercise, or do other activities that cause your oxygen saturation to fall.
Arterial Blood Gas Tests

Like pulse oximetry, the main purpose of taking an arterial blood gas test is to measure the amount of oxygen in your bloodstream. However, arterial blood gas tests are more precise and detailed than pulse oximetry, and they can tell you even more important information about your blood.
Arterial blood gas (ABG) tests not only measure your blood oxygen levels, but also the amount of carbon dioxide in your blood. These results reflect how efficiently your lungs can perform their primary function, which is to move these gasses to and from your bloodstream.
ABG tests also measure your blood's acidity, or pH, to determine whether or not it falls within a healthy range. Abnormal results can indicate too much carbon dioxide in your blood (aka hypercapnia), which is often caused by lung function decline.
With all these different measurements, arterial blood gas tests can give you a clearer picture of how gas exchange works in your lungs. It can also reveal problems like hypoxemia and help you pinpoint specific respiratory problems like poor oxygen absorption or carbon dioxide removal in the lungs.
Doctors generally use arterial blood gas tests instead of pulse oximetry whenever they need a more precise measure of your blood oxygen saturation. Unlike pulse oximetry, it also allows them test for high blood carbon dioxide levels, or hypercapnia, a potentially dangerous condition which is common in people with severe COPD.
Taking Arterial Blood Gas Tests

Unlike pulse oximetry, which is designed to be simple, non-invasive, and yield immediate results, arterial blood gas tests are somewhat more involved. ABG tests also require you to give an arterial blood sample, which can make them a bit more unpleasant to complete.
Unlike many other types of blood tests, ABG tests require blood to be taken from an artery instead of a vein. Many people find this to be more uncomfortable or painful because arteries tend to be surrounded by more sensitive nerves and tissues.
Fortunately, one quick and simple blood draw is all you have to go through in order to take an arterial blood gas test. Your doctor or nurse will take a small sample of blood from your arm or another major artery, and then your part of the procedure will be done.
If you use supplemental oxygen, your doctor will tell you whether or not you should use it before taking the test. If you can go without oxygen therapy for short periods of time, your doctor may ask you to stop using oxygen for about 20 minutes before drawing blood.
Once you've given your blood sample, your doctor will most likely need to send it off to another lab for analysis. If your doctor is lucky enough to have access to a blood gas analyzer on-site, he may be able to get your test results right away.
Interpreting Your Arterial Blood Gas Test Results
 |
| A measurement chamber used to analyze arterial blood samples. |
Arterial blood gas tests give you five main pieces of information about your blood:
- Blood pH
- Bicarbonate Levels
- Partial Pressure of Oxygen
- Partial Pressure of Carbon Dioxide
- Oxygen Saturation
In the following sections, we'll explain what each of these measures is and how to know if your results fall within the healthy range. But even though it's important to know how to read these reports yourself, only your doctor has the knowledge to fully interpret what they mean.
Partial Pressure of Oxygen and Carbon Dioxide

Partial pressure of oxygen is a measure that tells you how much oxygen you have in your bloodstream and is abbreviated PaO2. In order to be considered healthy, your PaO2 should be between 80 and 100 mmHg.
Similarly, partial pressure of carbon dioxide is a measure of how much carbon dioxide is circulating in your bloodstream, and is abbreviated PaCO2. The healthy range for PaCO2 is between 35 and 45mmHg, and it means that your lungs are able to process carbon dioxide efficiently.
This balance is important, and any abnormalities in your oxygen or carbon dioxide levels can lead to more severe respiratory problems. It can also cause blood pH imbalances like respiratory acidosis.
If your PaO2 is lower than 80, that means you have hypoxemia, which is often caused by poor lung function. A PaCO2 higher than 45mmHg means that you have hypercapnia, which means that your lungs are not removing enough carbon dioxide from your blood.
Hypercapnia is a sign of severe COPD, since it usually only happens when you experience prolonged lung function decline. In some cases, hypercapnia can be caused by supplemental oxygen therapy, especially if you are breathing in more oxygen than you should.
However, these numbers can reveal more than that, which is why they are more useful than a simple oxygen saturation measurement (SpO2). For instance, if you show signs of hypoxemia, comparing your PaO2 and your PaCO2 together, and with other test results, can give your doctor a better idea of the cause.
Hypoxemia is usually caused by one of several things, including hypoventilation, poor gas diffusion, or ventilation-perfusion mismatch. Hypoventilation results from breathing too shallow and slow, while ventilation-perfusion mismatch is a sign of more complex problems with gas exchange in the lungs.
Ventilation-perfusion mismatch is the most common cause of hypoxemia, and is common in people with COPD. But because these relationships are complicated, you will need your doctor to interpret the nuances of what your partial pressure of oxygen and partial pressure of carbon dioxide mean.
Oxygen Saturation
Your ABG test results will also show you your blood oxygen saturation, recorded as your SpO2. This is the exact same thing that a pulse oximeter measures, though the ABG test will likely yield a more accurate number.
You interpret this measure using the exact same criteria that you would use to interpret a pulse oximeter reading. An SpO2 greater than 95% is healthy, while anything less is a sign that your lungs are not able to absorb enough oxygen into your blood.
Blood pH

In order to be healthy, your blood pH must fall within in a very small range between 7.35 and 7.45. A pH that's too high is considered acidic, while a pH that's too low is considered alkaline.
If Your Blood is Too Acidic
If your blood pH is below 7.35, then that means it is too acidic. This is known as acidosis, but it can be further narrowed down to respiratory acidosis or metabolic acidosis depending on its cause.
To determine the cause, you need to compare your blood pH with the partial pressure of carbon dioxide in your blood, or your PaCO2. Low blood pH paired with a high PaCO2 is a sign of respiratory acidosis, while low blood pH paired with a low PaCO2 is a sign of metabolic acidosis.
Metabolic acidosis is usually caused by a metabolic disorder rather than a respiratory cause. It can signal a variety of problems, including diabetes, kidney or liver disease, extreme dehydration, or poisoning from aspirin, methanol, or ethylene glycol (a toxic chemical in antifreeze).
Respiratory acidosis happens when enough carbon dioxide (an acidic molecule) builds up in your blood to raise the pH above normal. This is usually caused by respiratory diseases like COPD, which can render your lungs incapable of removing carbon dioxide from your bloodstream quickly enough.
Respiratory acidosis is relatively common in people with COPD, especially those with severe lung function impairment. It's more likely to happen if you experience a COPD exacerbation or use supplemental oxygen to treat your disease.
Anyone who uses oxygen can experience respiratory acidosis as a side effect, but it is most likely to happen to those who misuse their oxygen therapy. If you use too much oxygen or don't follow your prescription carefully, it can disrupt the balance of gas exchange in the lungs.
If Your Blood is Too Alkaline
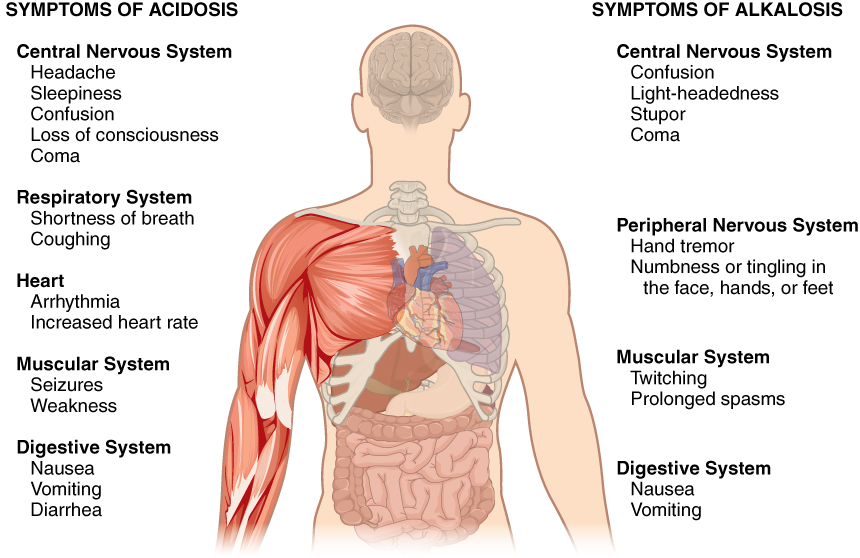
If your blood pH is higher than 7.45 then that means it is too alkaline. This is referred to as alkalosis, which is a relatively rare condition not associated with COPD or other lung diseases.
Unlike acidosis, alkylosis is caused by problems completely unrelated to respiratory problems or lung function decline. Instead, it is usually caused by kidney problems, dehydration, or temporary illnesses.
Bicarbonate Levels
Your bicarbonate levels tell you about your body's metabolism and specifically your kidney function. Healthy bicarbonate levels fall between 22 and 26 mmol/L.
Your doctor will correlate your bicarbonate levels with other information reported in your ABG test results (particularly your blood pH) to look for signs of kidney problems or other metabolic dysfunction. For instance, if you have metabolic acidosis (low blood pH and low PaCO2) and your bicarbonate levels are low, it indicates that excessive dehydration may be the cause.
Putting it All Together
All of these different measures only scratch the surface of what an ABG test can reveal. Your actual results will give your doctor a wealth of useful information than he can use to evaluate your respiratory health.
To truly understand what your ABG test results mean, you will have to ask your doctor to explain. Interpreting the results of an arterial blood gas tests is a complex and nuanced process that only a trained physician can understand.
To get the full picture, your doctor has to correlate all the different results along with additional information about your symptoms and your overall health. He also has to take a variety of complex relationships between the different measures into account.
While it helps to be familiar with the important terms and measures, you should always ask your doctor to walk you through your ABG test results. He can explain what each number means, how they are related, and what the results say about about your health and your COPD.
Understanding Your Chest and Lung Scans

Chest x-rays and CT scans are common procedures used to diagnose COPD and to monitor the disease long-term. Different types of scans produce different types of images, but both can reveal a variety of important things about your lungs.
In general, chest scans help your doctor get a better idea of your lung anatomy and the severity of your COPD. It also allows him to track any visible changes that happen to your lungs over time.
Here are some of the lung features and conditions that your doctor will look for on a chest scan:
- Enlarged or hyper-inflated lungs
- Pockets of air or fluid in and around the lungs
- A collapsed lung
- Pulmonary nodules (spots on the lungs)
- Signs of lung infection (e.g. pneumonia and tuberculosis)
- Lung structure changes caused by COPD (especially emphysemous tissue)
- Lung cancer (tumors)
- Flattened diagram
- Signs of heart disease and heart valve problems
- Certain other major changes to the structure of your heart and lungs
Chest X-Rays

X-ray scans use ionizing radiation to produce two-dimensional, black-and-white images of the major structures inside your body. Chest x-rays show the heart, lungs, upper airways, blood vessels, and all the bones in your chest cavity.
Doctors often use chest x-rays to diagnose people with severe respiratory symptoms and to monitor people with COPD. The images allow them view the structure of your organs and tissues to look for signs of disease and damage to your heart and lungs.
Chest x-rays also help your doctor monitor the condition of your heart and lungs long term. This allows him to track any changes, determine how well treatments are working, and judge how quickly the disease is worsening with time.
X-ray images tend to show some details and some types of tissues better than others, but you can always see the general shape and structure of the larger and denser tissues. In the case of COPD diagnosis and monitoring, your doctor will look specifically at your lungs for abnormalities.
He will also look for evidence of other problems that could be the cause of your respiratory ailments or worsening COPD symptoms. These include signs of heart disease, lung infections, lung cancer, and lung infections like pneumonia.
Taking a Chest X-Ray

Chest x-rays are quick, painless, and take minimal effort to complete. For the most part, all you have to do is stay still and strike a few poses while your doctor takes the images.
First, you will go to the x-ray exam room and remove your clothes and any jewelry you're wearing from the waist up. Afterward, your doctor will show you where to stand, sit, or lie near the x-ray machine.
Then your doctor will ask you to position your arms, shoulders, and body in specific ways so he can x-ray different areas and angles of your chest. He will take scans from the front and from the side, and he may also ask you to hold in deep breaths to help him get clearer images of your heart and lungs.
As you pose, your doctor will activate the x-ray machine to send out a quick pulse of ionizing radiation. Much of this radiation passes through your body and hits a metal x-ray plate behind you.
This radiation caught by the plate reveals valuable information about your insides because the denser structures in your body block more radiation than structures that are less dense. The machine is able to detect the amount of radiation that passes through different areas in enough detail to produce a black-and-white image of your insides.
The radiation itself is completely painless and nothing to be worried about; chest x-rays are just as safe as the routine dental x-rays you get at the dentist's office. Even getting frequent chest x-rays does not expose you to enough radiation to put your health at risk.
Interpreting Your Chest X-Ray
 |
| X-ray scan showing lungs with emphysema. |
You probably won't recognize much by looking at your x-ray scan on your own unless you're a certified radiologist. It takes a trained eye to make sense of the image and interpret what it means, and it's not something that most primary care doctors can even do on their own.
Most of the time, an experienced radiologist will analyze your x-ray scans for major features and abnormalities. Then, the radiologist will send his report along with the scans to your doctor, who will interpret the results within the context of the rest of the information he has gathered about your health.
While the scans probably won't look like much to you, your doctor can point out all the important features in the image if you ask. Once you know what it shows and what to look at, it will be easier to understand what they mean and how your doctor interprets the results.
Here are a few tips to help you figure out what you're looking at when you view your x-ray scans:
- The lightest colors on the image represent the densest structures inside your body, like your bones.
- The darkest colors on the image represent the lightest, least-dense structures in your body, such as the air space in your lungs.
- The middle tones, or gray colors, represent medium-density structures like fat and muscle.
Unfortunately, x-rays scans often cannot catch COPD in the early stages because the signs are subtle and x-ray images only reveal a limited amount of information about the lungs. It's usually not until the later stages of the disease, when the lungs are severely affected, that signs of COPD show up on an x-ray scan.
It's also important to realize that x-rays on their own generally don't reveal enough information to accurately diagnose and evaluate COPD. X-ray scans should always be interpreted alongside other information, including respiratory symptoms, lung function tests, and other exam results.
CT Scans

While x-rays are quick, simple scans, computed tomography (CT) scans are generally longer, more complex procedures. That's because CT scans capture your insides in much greater depth, showing all of your bones, organs, blood vessels, and soft tissues in more detail.
Like a chest x-ray, CT scans use bursts of ionizing radiation to capture images of your upper chest, specifically your heart and your lungs. However, CT scanners use a more sophisticated process to generate an accurate 3-D picture of your insides.
This is possible because a CT scanner takes many of individual pictures, each one showing one small cross-section of your chest. A cross-section image is like looking at a single, thin section of your body, just like taking a thin slice out of the middle of an orange allows you to see a cross-section of its insides.
When you put all of these cross-sections together in order, it produces what is essentially a detailed, three-dimensional model of all the major organs and tissues inside your chest. Your doctor can analyze this 3-D representation to see all kinds of anatomical details, which allows him to more accurately evaluate the condition of your heart and lungs.
Taking a CT Scan

When you go to get your CT scan, you will most likely need to go to a separate hospital or radiology clinic instead of your usual doctor's office. Most of the time, you will also need to fast from food and water for at least several hours before the test.
Compared to taking a chest x-ray, taking a CT scan often takes more time and preparation. One reason for this is that, in many cases, you will need to receive an IV containing a chemical dye (called a contrast chemical) to help the scanner see your insides better.
Another difference is that, instead of standing in front of an x-ray plate, you will have to lie down inside the CT machine during the scan. Some people find this part of the process claustrophobic, but it usually only takes a few minutes to complete.
If your scan requires and intravenous contrast chemical, your doctor or nurse will place an IV (usually in your arm) to dispense the dye shortly before your CT scan. You might also receive another medication to reduce the risk of any side-effects from the injection.
The IV placement, if you receive one, is by far the worst part of the procedure; it can cause discomfort at the injection site, an uncomfortable burning sensation, nausea, and other side effects. However, the dye is often necessary to make your lungs and other structures show up clearly on the scan.
The contrast chemical works by traveling through your bloodstream, where it gets absorbed by certain cells and tissues in your body. The cells containing the contrast chemical are easy for the scanner to pick up, causing the dyed tissues (e.g. your lungs) to appear more clearly and prominently in the image produced by the scan.
Once the contrast chemical has had enough time to work, you will go to the exam room where the actual CT scanner is. While you usually don't have to remove all your clothes, you will need to remove anything containing metal, including glasses, jewelry, hearing aids, dentures, and metal underwire bras.
The CT scanner itself will look like a large, square or donut-shaped machine with a circular opening in the middle attached to a rectangular bed. To do the scan, you will need to lie down on the bed inside the circular opening while the scanners, containing x-ray emitters and receivers, rotate around the outside.
While you lie in the CT machine, the scanners emit bursts of x-ray radiation on all sides of your body in order to get a complete image of your chest. The bed also moves forward and backward to position the correct parts of your body within the scanning area.
Depending on the procedure the CT machine uses, it can take 30 seconds to several minutes to complete the scanning process. However, you may need to repeat the scan more than once to get a clear enough picture from the machine.
In order to prevent the image from blurring, you will need to stay completely motionless during the entire scan. You may also need to hold your breath or have parts of your body strapped down to help you keep yourself totally still.
Interpreting Your CT Scan
 |
| One cross-section from a CT scan showing a collapsed lung (right). |
Just like chest x-rays, CT scans are too complicated to interpret without proper training. However, with your doctor's help, you can better understand what's important about the image and how your doctor analyzes the results.
When evaluating your CT scan, your doctor and radiologist will look for many of the same features that they look for on an x-ray scan, including lung infections, tumors, and emphysemous tissue. The difference is that the CT images show much more detail, allowing for more precise evaluation and diagnosis.
CT scans can reveal many types of damage to the lung, including structural damage and deformities caused by COPD. Because of this, your doctor may want you to take CT scans at regular intervals (e.g. once per year) so he can track the progression of your disease.
Conclusion
Frequent doctor's appointments and medical tests are an inevitable part of living with COPD. But even though this can be frustrating or inconvenient at times, it is a necessary and vital to get adequate treatment for the disease.
However, you might find the process less tedious if you can analyze and understand your test results yourself. This will not only help you understand your disease better, but it also allows you to take a more pro-active role in your treatment overall.
Now that we've explained how to interpret the most common COPD tests and health screenings, it's up to you to put that knowledge in to action. To do so, you will need pay attention and be an active participant during all your medical appointments.
Vital information about your health shouldn't be left in your doctor's hands alone; you deserve to know everything your doctor analyzes and discovers. Never be afraid to ask your doctor to see your test results or to explain them and go over them with you.
